
Decreased LOC
Quick Hits
An approach to decreased LOC at music festivals
Author: Dr. Caroline Gardiner
Editors: Drs. Brendan Munn, Qadeem Salehmohammed & Megan Singh
© Allen McEachern
Background
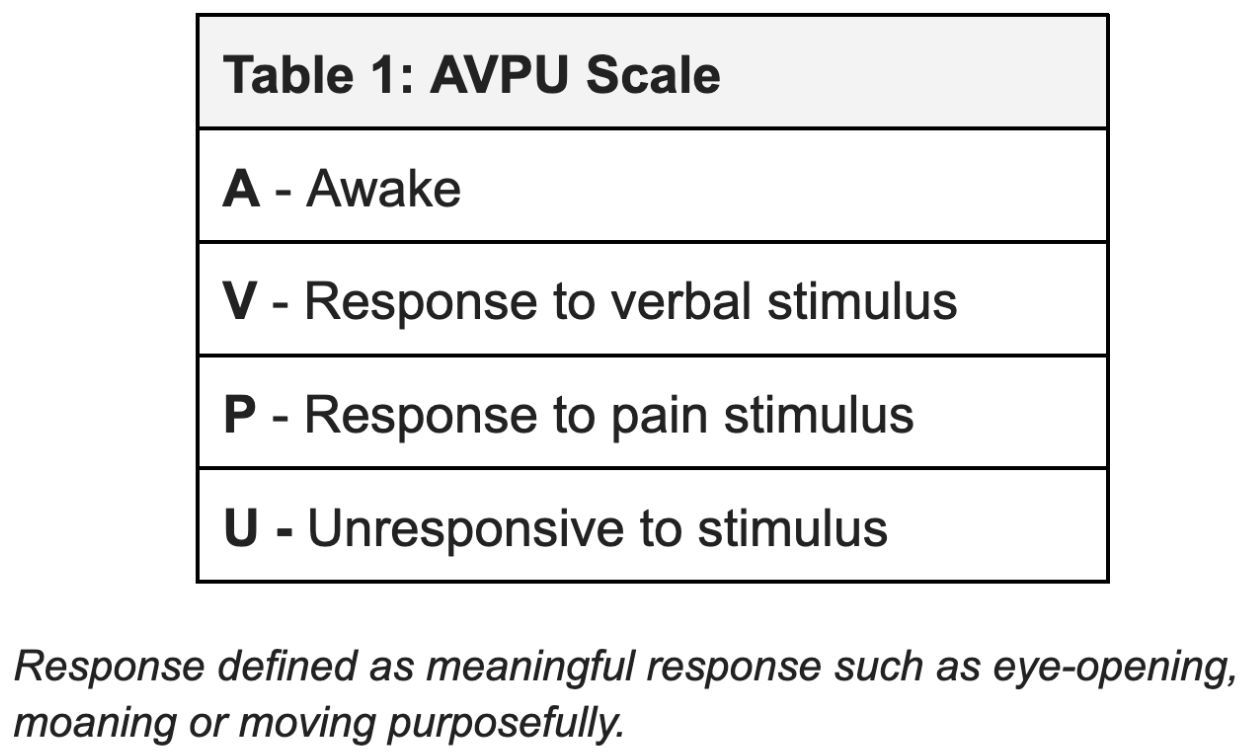
Decreased level of consciousness (dLOC) is an important presentation at music festivals (MFs). Although the cause is commonly intoxication with alcohol or other recreational substances, a number of important causes need to be ruled out, particularly when observing and recovering patients on site. Historically, large influxes of patients with dLOC have profoundly affected local health services. While providing care at events can decrease this potential impact, particularly on ambulances and hospitals, preparation with skilled personnel and equipment is needed to safely manage cases without transfer. Harm reduction and education efforts play a major role in decreasing both the volume and acuity presenting at medical services. dLOC is defined here as less than normal level of arousal (Glasgow Coma Scale of GCS ≤ 13 or P or U using AVPU Scale, see Table 1).
Alterations of Consciousness
Cases of dLOC comprise a subset of presentations of Altered Mental Status (AMS) that deals predominantly with disorders of consciousness or arousal. Changes in behaviour, affect, thought and cognitive function are forms of AMS discussed in the QH Agitation and QH Psychosis pagea. dLOC at MFs can present as several distinct clinical syndromes; these include transient (eg. syncope), short (eg. post-ictal), fluctuating (eg. GHB intoxication), or prolonged (eg. sedative/hypnotic overdose) courses. Please see QH Syncope and QH Seizure for the first two. The focus in this quick hit is on fluctuating and persistent dLOC - particularly profound coma states.
Evaluation of dLOC
Frequently, the GCS is used to assess dLOC; however, it was developed for traumatic brain injury (TBI). The “GCS less than 8, intubate” dogma comes from closed head trauma literature. Its application has been questioned in the toxicologic (particularly recreational) population. Applying this cutoff could result in rapid exhaustion of resources, and incur unnecessary intubation risk.
Other scoring systems, particularly AVPU, offer advantages at events. AVPU is favoured for simplicity and speed. It has good correlation with GCS and greater inter-rater reliability.
History
Onset and course of symptoms
Recreational substance history
PMHx
Medication history (especially anti-psychotics, SSRIs/MAOIs, anti-epileptics, opioids, benzodiazepines/sedatives)
Physical Exam
ABCs
Vital signs, including temperature and glucose
Trauma exam
Neuro exam
GCS/AVPU (noxious stimulus, ie. jaw thrust for 10s)
Pupils
Focal neurologic deficits
Investigations
Glucose
Sodium
Differential Diagnosis
The DIMS mnemonic is commonly employed for altered LOC and stands for Drugs, Infection, Metabolic and Structural causes. Young healthy populations at music festivals are more likely to be affected by drugs or specific ‘IMS’ diagnoses per the following list:
D: opioids, GHB, ketamine, ETOH, benzo, etc.
IMS:
Hypoglycemia
Hyponatremia
Seizure/post-ictal
Heat-related illness
Management
ABCs
Airway support as required (jaw thrust, OPA, etc)
Suction as required
Recovery position
Supplemental O2 to achieve SpO2 > 92%
IV access +/- fluid bolus
For concerning patients (GCS ≤ 8, supplemental O2, etc.)
Continuous pulse oximetry and 1:1 care
Nearby airway equipment and RSI drugs
For patients who return to baseline after a period of monitoring, have an identifiable underlying cause, are well supported at the MF, potential D/C
On-Site Observation
The majority of MF presentations with severe dLOC (GCS ≤ 8 or U) had intoxication from GHB. Cited case series have found that most patients in the ED and at MFs with GCS ≤ 8 recovered to a normal LOC within 3h, and all recovered within 6h. There is emerging evidence that observation of select intoxicated patients with dLOC is safe and advantageous. However, this conservative approach requires close observation in a monitored setting.
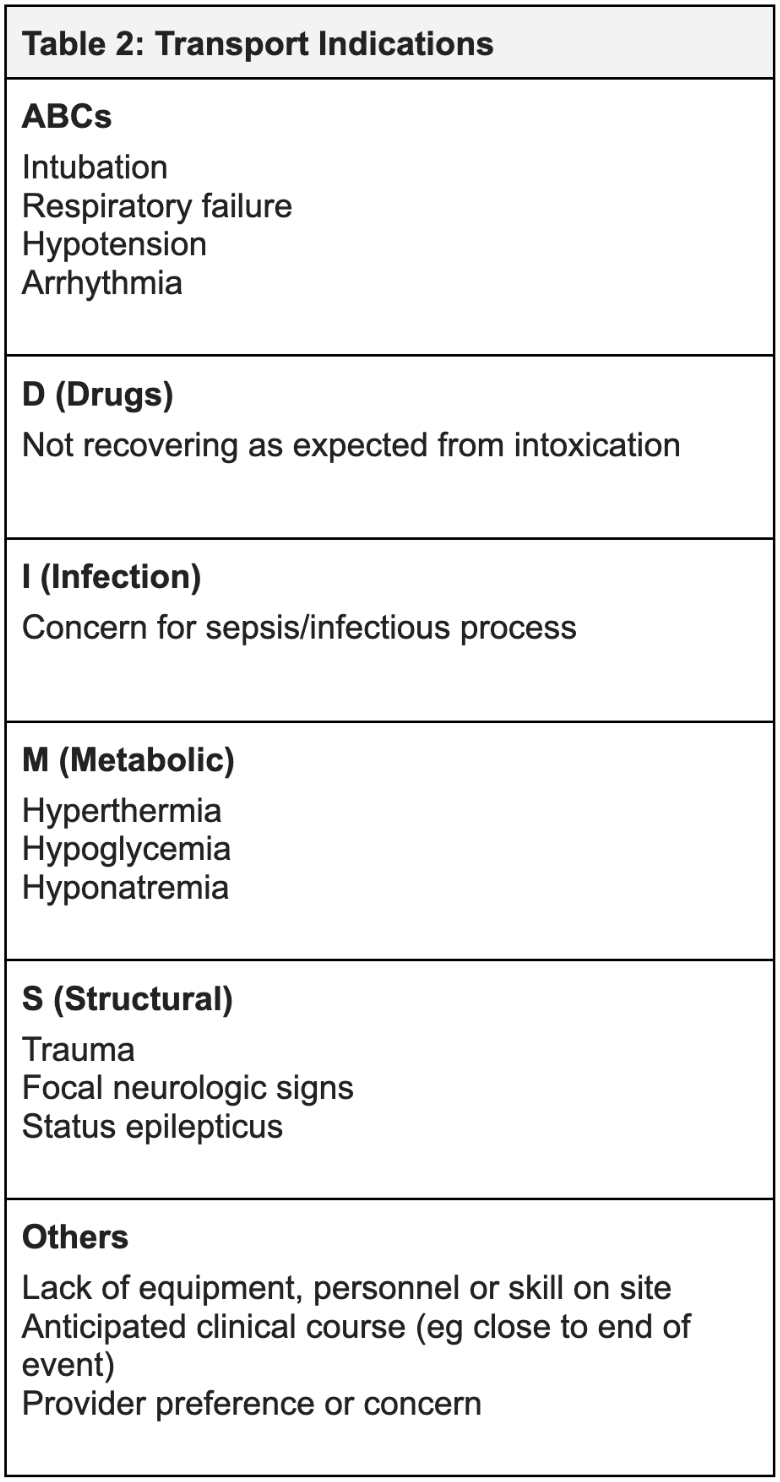
Acute intracranial processes (including trauma or seizure), as well as hyponatremia and hypoglycemia, must be ruled out. Indications for transport off-site are found in Table 2.
RESOURCES // REFERENCES
CrackCast Show Notes – Depressed Consciousness and Coma – August 2019 https://canadiem.org/crackcast
Resident Survival Guide: Red Book, McMaster Internal Medicine Residency Training Program, 8th edition
Life in the Fast Lane: GCS https://litfl.com/glasgow-coma-scale-gcs/
Forsberg S, Höjer J, Enander C, Ludwigs U. Coma and impaired consciousness in the emergency room: characteristics of poisoning versus other causes. Emerg Med J. 2009 Feb;26(2):100-2. doi: 10.1136/emj.2007.054536. PMID: 19164617.
De Paepe P, Lemoyne S, Buylaert W. Disorders of consciousness induced by intoxication. Neurol Clin. 2012 Feb;30(1):359-84, x-xi. doi: 10.1016/j.ncl.2011.10.003. PMID: 22284068.
Duncan R, Thakore S. Decreased Glasgow Coma Scale score does not mandate endotracheal intubation in the emergency department. J Emerg Med. 2009 Nov;37(4):451-5. doi: 10.1016/j.jemermed.2008.11.026. Epub 2009 Mar 9. PMID: 19272743.
Freund Y, Viglino D, Cachanado M, et al. Effect of Noninvasive Airway Management of Comatose Patients With Acute Poisoning: A Randomized Clinical Trial. JAMA. 2023;330(23):2267–2274. doi:10.1001/jama.2023.24391
Dietze P, Horyniak D, Agius P, Munir V, Smit de V, Johnston J, Fry CL, Degenhardt L. Effect of intubation for gamma-hydroxybutyric acid overdose on emergency department length of stay and hospital admission. Acad Emerg Med. 2014 Nov;21(11):1226-31. doi: 10.1111/acem.12516. PMID: 25377399.
Orso D, Vetrugno L, Federici N, D'Andrea N, Bove T. Endotracheal intubation to reduce aspiration events in acutely comatose patients: a systematic review. Scand J Trauma Resusc Emerg Med. 2020 Dec 10;28(1):116. doi: 10.1186/s13049-020-00814-w. PMID: 33303004; PMCID: PMC7726605.
van Helmond LPFM, Gresnigt FMJ. Safety of withholding intubation in gamma-hydroxybutyrate- and gamma-butyrolactone-intoxicated coma patients in the emergency department. Eur J Emerg Med. 2020 Jun;27(3):223-227. doi: 10.1097/MEJ.0000000000000649. PMID: 31815871.
Ribeiro SCDC. Decreased Glasgow Coma Scale score in medical patients as an indicator for intubation in the Emergency Department: Why are we doing it? Clinics (Sao Paulo). 2021 Mar 8;76:e2282. doi: 10.6061/clinics/2021/e2282. PMID: 33681943; PMCID: PMC7920397.
ED altered LOC papers
Calle P, Sundahl N, Maudens K, Wille SM, Van Sassenbroeck D, De Graeve K, Gogaert S, De Paepe P, Devriese D, Arno G, Blanckaert P. Medical Emergencies Related to Ethanol and Illicit Drugs at an Annual, Nocturnal, Indoor, Electronic Dance Music Event. Prehosp Disaster Med. 2018 Feb;33(1):71-76. doi: 10.1017/S1049023X17007099. Epub 2017 Dec 29. PMID: 29284546.
Munn, Matthew & Laraya, Jose & Lund, Adam & Turris, Sheila. . Altered Mental Status at Music Festivals: A Case Study Examining Clinical Concepts and Controversies. Prehospital and Disaster Medicine. (2017). 32. S131-S132.