
Airway
Quick Hits
An approach to the airway at music festivals
Author: Dr. Brendan Munn
© Allen McEachern
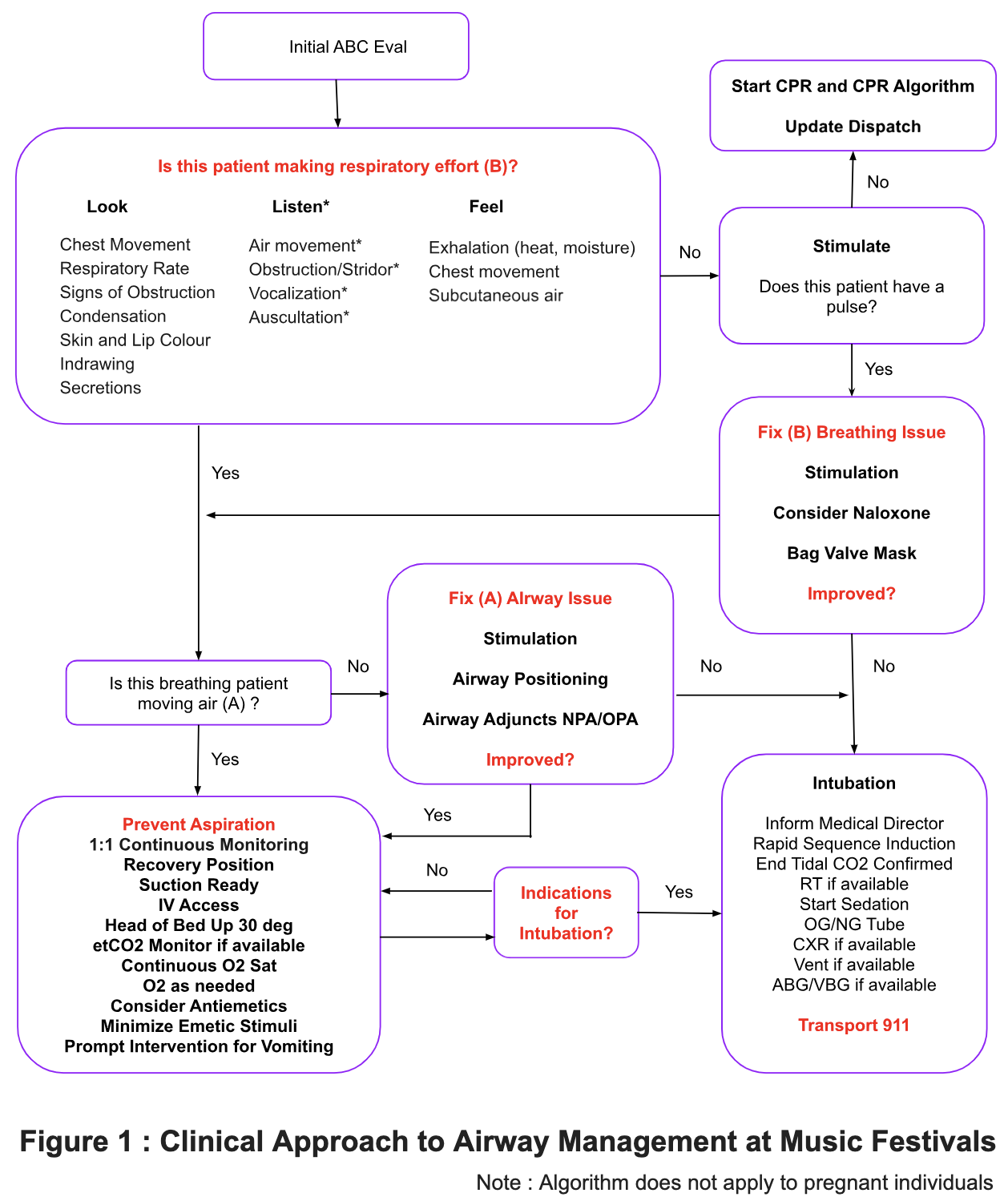
The Airway Algorithm
Background: Airway management is a critical skill at music festivals (MFs) due to the presence of potential full stomachs and altered mental status (AMS). Although airway complications and aspiration are rarely reported as primary causes of death, they are likely contributors in the context of recreational drug toxicity as a secondary precipitant of respiratory and/or cardiac arrests. Specific guidance for airway management and mitigation of aspiration risk at MFs is limited; most evidence is based on the toxicology and anesthesia literature, with extrapolations from prehospital data, ED sedation and postanesthetic care experience.
Basic Airway: The evaluation of AB (Airway and Breathing) in the festival environment is challenging due to factors like loud music, lack of / strobing of lights, crowds and AMS. The Look Listen* and Feel approach (see Figure 1) can be tailored to this unique space. Basic airway skills are paramount. Often underrated in the hospital environment, they are likely one of the most effective diagnostic and pathway-defining tools; this AB process often occurs at a critical (and brief) window for intervention. Luckily, attendees by and large are young and healthy, with normal BMI, airway anatomy and cardiorespiratory physiology at baseline. The vast majority of intoxicated patients are still breathing spontaneously and need little beyond supportive monitoring. Application of a painful stimulus (trapezius squeeze or finger pressure behind the angle of the jaw) is great for initial evaluation of the AV*PU scale; it also provides potential resuscitation if either A or B are found to be abnormal. See Table 1 for interventions. Overall, experience shows that advanced interventions are needed only in a small minority of patients.
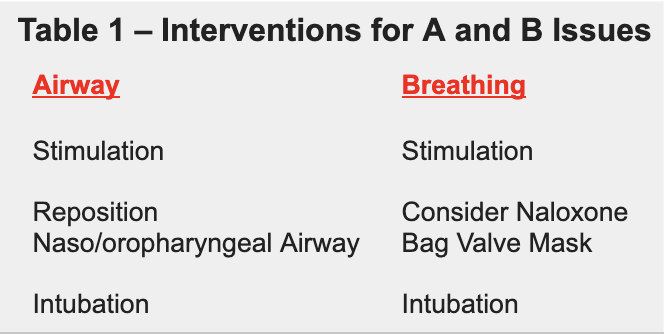
Aspiration: Aspiration is a major risk at MFs. Like pregnant women – the quintessential patients at risk of aspiration – intoxicated patients at MFs require adapted and reasoned care. True aspiration requires alignment of a “swiss cheese” series of events where stomach contents, regurgitation and loss of airway reflexes result in entry into the bronchial tree with clinically significant pneumonitis and/or loss of ventilatory volume. The combination of potential full stomachs, altered mental status (AMS) and our own therapeutic interventions means that the risk of this complication can be minimized through careful selection of interventions and avoidance of emetic stimuli. This is reflected by unpublished field experience where stimulation, recovery position and airway repositioning are used an order of magnitude more than airway adjuncts; furthermore the use of nasopharyngeal over oropharyngeal airways, the avoidance of gag reflex testing and bag valve mask / positive pressure ventilation entirely – and gentle low pressures when used at all – all aid in decreasing the risk. There is some suggestion that deep loss of consciousness is protective, with the middle range of Glasgow Coma Scales (GCS 5-13, especially while upward on emergence) being the most risky period.
Intubation: The decision to intubate is a risk/benefit evaluation that must be made for each individual patient. In general at MFs, less is more in people who are stable and spontaneously breathing recognizing that intubation has associated risks particularly in an out of hospital, austere or remote setting. In select patients, intubation is often not indicated or necessary despite GCS < 8 and provider apprehension. Evidence and experience is emerging in support for selective non-intubation and close continuous monitoring in select patients. Research has postulated the advantages to avoiding intubation in case series and emergency department practice.
Management: The focus is on (a) promptly identifying and correcting abnormalities of A&B, (b) treating and minimizing patient and provider risk factors for aspiration, and (c) identifying appropriate patients for close and continuous monitoring and observation. See Figure 1 for an algorithm outlining this approach.
Ensure to consider an approach for these key questions:
Is this patient making respiratory efforts?
Is this patient moving air?
Does this patient need basic interventions?
Is this patient likely to benefit from intubation?

The Recovery Position
References
Orso et al. Endotracheal intubation to reduce aspiration events in acutely comatose patients: a systematic review. Scand J Trauma Resusc Emerg Med. (2020)
Aldrich T et al. Aspiration after overdosage of sedative or hypnotic drugs. South Med J. (1980)
Adnet F, Baud F. Relation between Glasgow Coma Scale and aspiration pneumonia. Lancet. (1996)
Liisanantti J et al. Aspiration pneumonia following severe self-poisoning. Resuscitation. (2003)
Isbister GK et al. Aspiration pneumonitis in an overdose population: frequency, predictors, and outcomes. Crit Care Med. (2004)
Dietze P et al. Effect of intubation for gamma-hydroxybutyric acid overdose on emergency department length of stay and hospital admission. Acad Emerg Med. (2014)
Duncan R, Thakore S. Decreased Glasgow Coma Scale score does not mandate endotracheal intubation in the emergency department. J Emerg Med. (2009)
Vaughan GG et al. The prevention and treatment of aspiration of vomitus during pharmacosedation and general anesthesia. J Oral Maxillofac Surg. (1992)
Munn MB et al. Altered Mental Status at Music Festivals: A Case Series Examining Clinical Concepts and Controversies. Prehospital and Disaster Medicine. (2017)
Munn MB et al. Canadian emergency physician attitudes toward endotracheal intubation for aspiration prophylaxis. CJEM. (2020)
Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obstet Gynecol. (1946)
NAP4 : The National Audit Project of the UK Royal College of Anaesthetists and The Difficult Airway Society. 2011.
Schwartz et al. Death and other complications of emergency airway management in critically ill adults. A prospective investigation of 297 tracheal intubations. Anesthesiology. (1995)