Agitation
Quick Hits
An approach to agitation at music festivals
Authors: Drs. Devon Mitchell & Ian Cooper
Editors: Dr. Brendan Munn
© Allen McEachern
Background
Agitation is a common presentation at music festivals (MFs) due to environmental factors such as dehydration and sun exposure, as well as substance use. Agitation as a medical entity exists on a spectrum of disease from mild agitation to hyperactive delirium with severe agitation; as with all causes of altered mental status (AMS), causes can be grouped into four wide categories (Drug-related, Infectious, Metabolic and Structural) using the DIMS mnemonic.
Agitation at Music Festivals
Although substance use is common in the festival environment, it is important not to inappropriately anchor on the diagnosis of substance intoxication. Agitated patients can be difficult to manage in the festival environment, amplifying the difficulty of the usual pre-hospital setting. Not all agitation is life threatening, but if not recognized and treated it can become a serious concern.
Approach and Initial Management
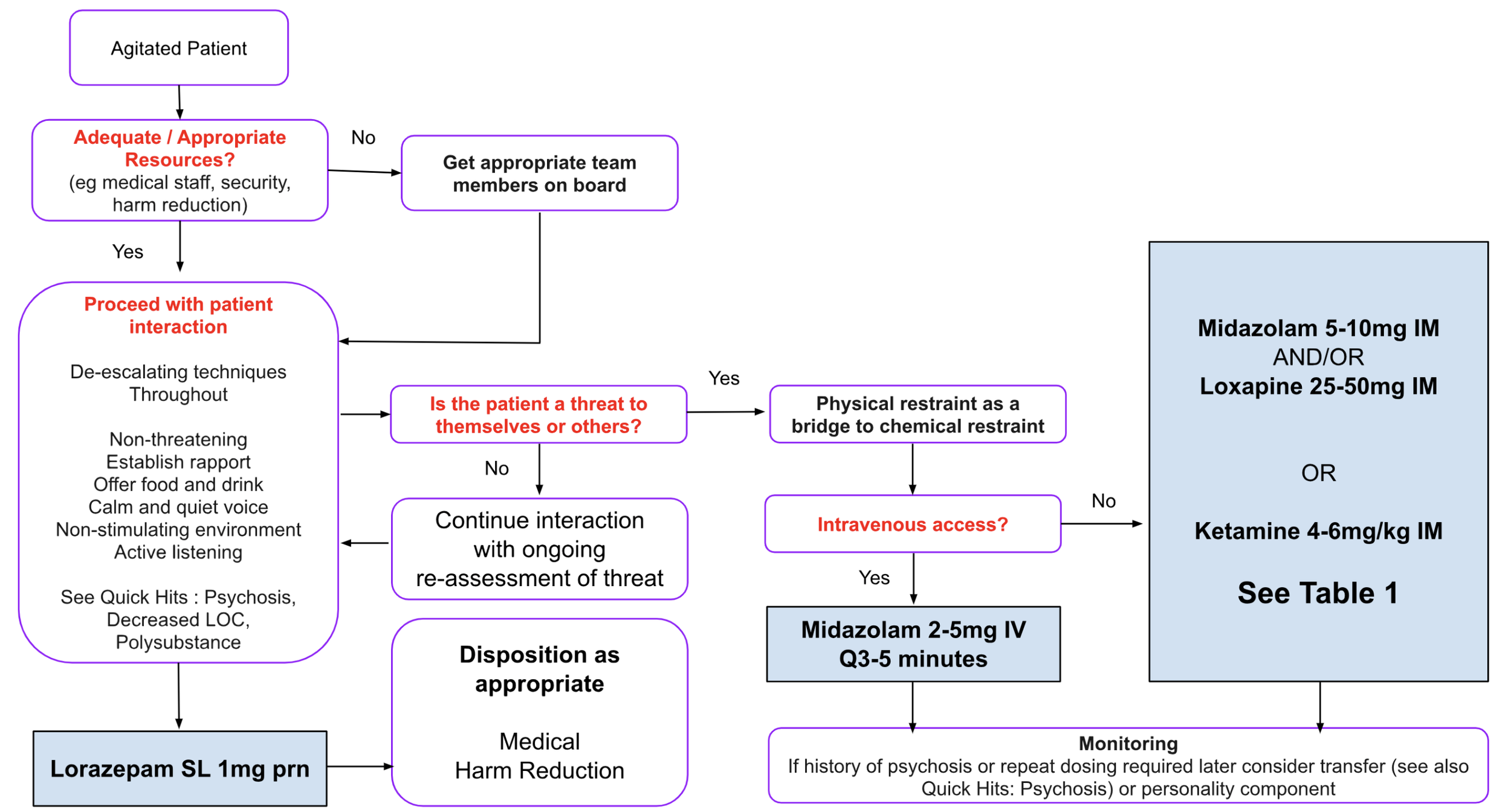
Management priorities are dictated by the severity of the agitation, and are outlined in the algorithm found in Figure 1. For mildly agitated patients, a non- confrontational manner and verbal de-escalation techniques can be all that is needed. Offering food and drink, establishing a quiet or restful environment, speaking in a calm and quiet voice, while establishing rapport and listening in attentively. Having security services trained for this population can greatly help to avoid escalation, and often there are other on-site services (harm reduction, festival health, chill zones, psychedelic support, etc) that can be invaluable for support and dispositioning. Sublingual benzodiazepines (eg lorazepam) can help to calm and reassure patients and prevent worsening. For violent or threatening situations the safety of providers, bystanders and the patients themselves is paramount. Physical and chemical restraint (P&CR) may be warranted if resources, skill and monitoring capabilities allow. This process is beneficial despite its inherent risks, and literature supports prehospital and use at MFs when warranted.
Excited Delirium
This clinical triad (severe agitation, adrenergic overdrive and forcible restraint resulting in cardiac arrest) has been controversial and lacks a clear definition. Nevertheless, the preferred approach in this scenario is rapid chemical restraint with cardiorespiratory support and monitoring.
Approach to Agitation at Music Festivals
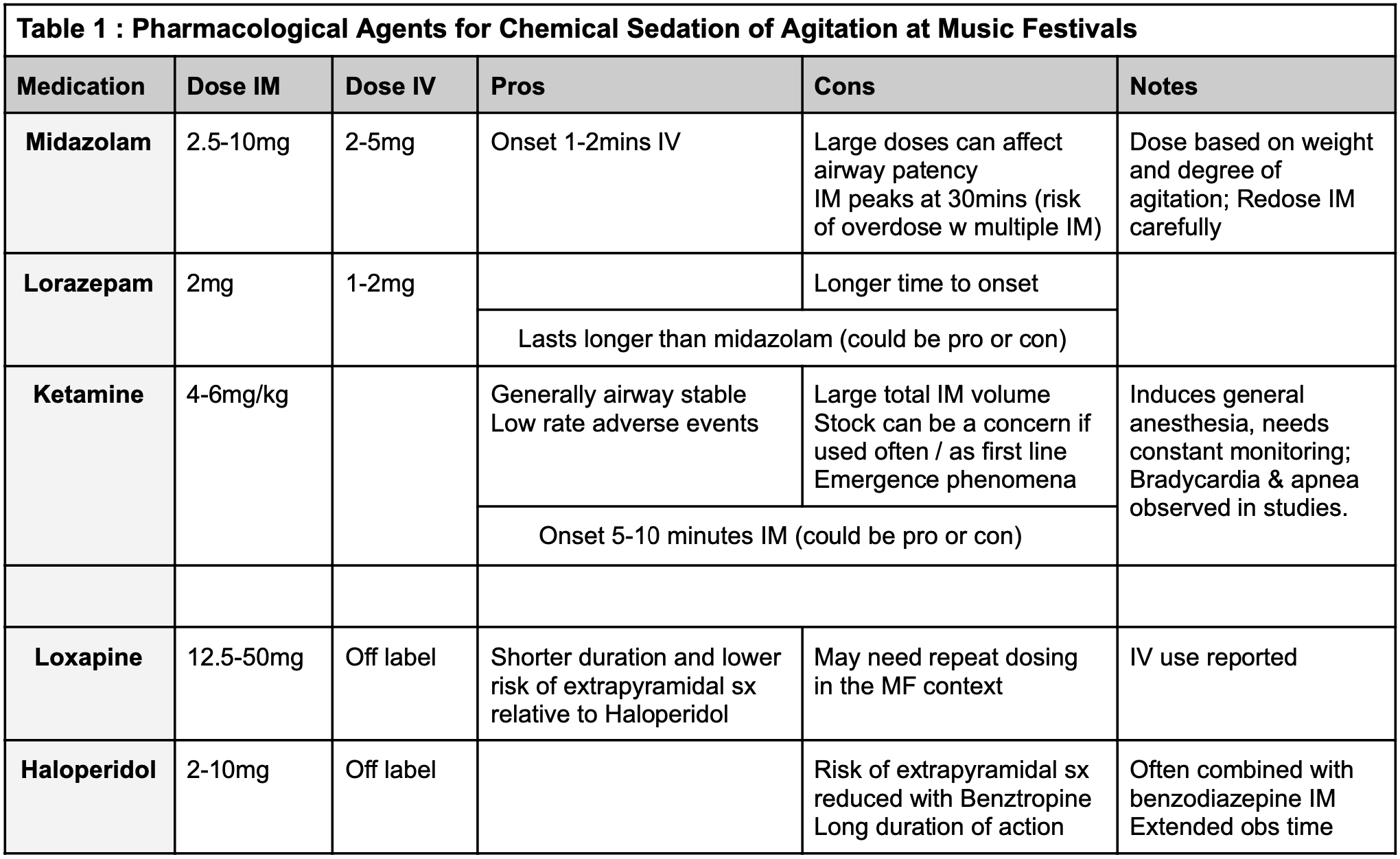
An algorithmic approach to the evaluation of agitation is found in Figure 1. Physical restraint should be employed as a bridge to chemical restraint only to prevent physiologic derangements (rhabdomyolysis, electrolytes or respiratory compromise) leading to cardiac arrhythmia and death. 4-point restraints for ankles and wrists as well as the more effective Pinnel restraints (with shoulders and waist) can be used. Keep in mind that involuntary restraint is also damaging to the mental health of patients, particularly while under the influence of stimulants. There are a variety of pharmacological agents available for chemical restraint, each with their own pros and cons. A summary of these is found in Table 1.
History
Often difficult to obtain, absent and/or limited
Collateral from friends or bystanders if available
Substance use Hx, if available
PMHx and medication history, if available
Physical
ABCs and vitals
Restraints, especially if affecting ABCs
Trauma exam (head injury or secondary trauma)
Neurologic exam (pupils, tone, LOC, focal deficit)
Investigations
Glucose
Electrolytes, especially sodium
VBG if available for metabolic acidosis
Differential Diagnosis
Drug Intoxication
Sympathomimetic, Serotonin Syndrome
Hallucinogenic
Infection (rare)
Trauma
Postictal State
Metabolic
Electrolytes (Sodium) or Hypoglycemia
Hyperthermia
Personality
Figure 1. Clinical Approach to Patient with Agitation at a Music Festival